What is ADA?
ADA stands for Alternatives to Domestic Aggression. ADA is a program that specializes in working with men and women to stop their use of abuse. The purpose of ADA is to end domestic violence and abuse in our community.
How does a man get into ADA?
By calling 734.971.9781 Ext. 430 for an application packet, completing the application and returning it to ADA in the self addressed stamped envelope included in the application packet. Please see the Services and Forms page.
How does a woman get into ADA?
By calling 734.971.9781 Ext. 468 to schedule an intake with the RENEW Coordinator or visiting our RENEW page.
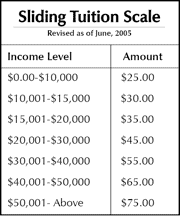
How much does it cost to go to ADA?
Tuition is based upon income. Below, you can see the sliding tuition scale. Assessment appointment fees are determined on a slightly different scale.
Is this program confidential?
Yes. Like all social service professionals, we maintain the confidentiality of service participants. There are circumstances when we are ethically bound to convey confidential information about service participants. Examples of this include when it is believed that children are being abused/neglected, or when we believe the service participant is an imminent threat to someone.
How long is the ADA program?
The ADA program is a minimum of 52 weekly sessions. Groups meet for two hours and are offered in both the morning and evening. Referrals can be made to the ADA Program for any duration.
What is the design of the ADA program?
Please visit the Services page for an outline of the ADA program.
Does ADA offer individual counseling for men who batter?
Yes. We do offer individual counseling. However, this is generally in addition to group intervention, not instead of. Group intervention has proven to be the most effective modality for those who use abuse or violence on their family. Many couples seek marital/couple counseling because they think the problem is one of communication. This is not the case. The perpetrator as a means of controlling his partner will utilize domestic violence tactics. Marital counseling, in cases where there is domestic violence, puts the woman at risk for further abuse. People who abuse need to be in group intervention programs with other abusers. Couples counseling is NEVER an appropriate way to deal with domestic violence. Therapists who offer couples counseling when domestic violence has occurred or is occurring do not understand the dynamics of domestic violence, and are practicing unethical and unsafe services.
Can I refer someone to ADA for assessment only?
Yes. We can report our conclusions and/or status of a referral to anyone for whom a service participant has signed an information release authorization.
Does ADA offer services to women who assault their male partners?
Yes! We specialize in offering these services to men AND women. See our RENEW page.
Are all the participants in ADA court ordered?
No, however about 85%-95% of the participants in ADA are court ordered. The rest are what we call “circumstance ordered”, “socially mandated” or “consequence ordered”. We say this because many men in particular come to ADA as a way to save their marriage, keep their partners from leaving, pressure their partners to return if they have already left, manipulate the court regarding child custody or visitation, or to avoid other unwanted circumstances. ADA’s goal is NOT to “save” or “end” relationships – it IS to end his violence and/or abuse.
Who is an appropriate referral to ADA?
If you are concerned about being abusive with your partner, ask yourself these questions and consider them as the warning signs of a problem.
- Was there violence in your family?
- During conflict do you often threaten an individual, break things, punch walls, slam doors, ignore the individual, or leave?
- Do you have mood swings, where one moment you feel loving and affectionate, the next moment angry and threatening?
- Have you ever used physical violence (shoved, grabbed, hit, slapped, strangled, etc.) on your partner, or any past partners?
- Do you tend to blame others for your behavior, especially your partner?
- Are you a jealous person?
- Do you try to control how your partner thinks, dresses, who she sees, how she spends her time, how she spends her money?
- Do you try to discourage her from seeing her friends or family?
- Do you get angry or resentful when she is successful in a job or hobby?
- Do your conversations quickly escalate into threats of separation or divorce?
- Do you ever threaten to hurt her, yourself, or others, if she talks about leaving you?
- Do you do or say things that are designed to make her feel “crazy” or “stupid”?
- Do you blame alcohol, drugs, stress, or other life events for your behavior?
- Do you feel guilty after your aggressive behavior and strive for her forgiveness?
- Do you think that you could never live without her, yet other times want her out of your life?
- Do you use sex, money or other favors as a way to “make up” after conflict?
- Is your partner afraid of you sometimes?
- Have you ever said “don’t make me angry”?
Why does ADA conduct drug and alcohol assessments?
Research indicates that approximately 55% of batterers/abusers have a history of problems with alcohol or other drugs. ADA staff must be aware of this history in order to provide the most effective services. Please note that alcohol or other drug intoxication or problems NEVER cause domestic violence. To offer treatment only for alcohol or other drug problems will neglect the dynamics of domestic violence and the battering or abusive behavior will continue.
An extensive list of resources on the relationship between drugs/alcohol and domestic violence (pdf)
Does ADA serve gay/lesbian batterers/abusers?
Yes. Gay/lesbian batterers/abusers can be seen on an individual basis or in the ADA batterer intervention groups.
Why do participants drop out of ADA?
Many choose to drop out of ADA when they learn that they will be held accountable for their abusive behavior. The ONLY reason people drop out of ADA is because they have made the decision to continue their abusive behavior, although their excuses will vary. Here is a list of some of the common excuses men frequently use when they choose to drop out of the program:
- “My tuition is too high”
- “They don’t have reasonable hours”
- “Those facilitators are too strict”
- “I don’t want to do it if I have to be in a group”
- “The facilitators don’t understand our situation”
- “I’m not as bad as the rest of the men in the group”
- “The facilitators blame men for everything!”
- “The attendance policy is unreasonable”
- “I’m better now”
- “The facilitators think I have an alcohol or drug problem and I don’t”
- “The facilitators only concentrate on the bad, not the good”
- “This is a relationship problem, I don’t have a problem”
What is ADA’s success rate?
Ultimately, ADA is as successful as each individual is committed to changing their life. We offer specialized intervention services to men and women. If they choose to use our services, they can change their behavior, attitudes and thinking. If they are committed to avoiding change, they will be successful in avoiding change.
What is the recidivism rate for batterers?
Measuring recidivism can be difficult, since there are many types of violence which are not easily tracked. Physical violence is the most measurable type of domestic violence because if often results in arrests and the event can then be quantified. However, other types of abuse, control and violence which may not be illegal are not easily quantified or tracked. Participants who come to ADA are only here for two hours per week. Knowing what their activities are outside of group and knowing how they are being abusive after leaving ADA is difficult to gauge unless they are rearrested. Someone could be verbally abusive and controlling without being arrested.
Why did we stop taking Insurance for Service Participants in the ADA Program?”
History: When we began the ADA Program in 1986 our philosophy and practice were evolving. This philosophy initially grew out of our clinical practice and training. Clinical practice is wholly different from batterer intervention work as we know it today. Today, we do not call what we do “treatment” or “counseling” we call it intervention. Intervention is about education, consequences, confrontation, acknowledgment, identification, etc.
Philosophy: We believe that battering is about the conscious, intentional and premeditated act to control and dominate another person. Battering is instrumental behavior. This is not a diagnosable “ailment” any more than bank robbery or speeding in an automobile is. Further if indeed an individual has a diagnosable illness/condition they would require proper treatment for that. Battering is not an illness or a condition.
Diagnosis: In order to bill an insurance company for services there must be a diagnosis for the “patient” there is no diagnosis for an individual who chooses to dominate and control an intimate partner. If, for example, we were to diagnose an individual as having an Intermittent Explosive Disorder there would be a number of problems.
- To begin with, according to the DSM-IV this disorder is “apparently rare”
- Given our philosophy (that battering is a choice which the batterer makes) we would not be offering treatment for this diagnosis, thereby committing insurance fraud, i.e. The treatment you offer must be for the disorder you are diagnosing
- An Intermittent Explosive Disorder is classified as an Impulse Disorder — Battering is not caused by an impulse disorder
Law: Most insurance company policies state that they will not cover court ordered treatment. Often times the provider and the company collude to look the other way and not document the court ordered aspect of the treatment.
Consequences: We believe that consequences* (not punishment) are a cornerstone of what is necessary to stop battering. It just does not make sense that a consequence for committing a violent crime could be covered by the benefits of employment/insurance.
Cost: The cost of maintaining a psychiatrist, keeping up with the immense demands of record keeping necessary for insurance billing compared with the revenue generated from the insurance reimbursement was prohibitive. Further our sliding scale ability made it feasible for service participants to pay approximately the same tuition as their co-pay. The trend in the insurance industry is towards treatment of an extremely “shorter duration” than we believe necessary for individuals who batter.
*Consequences should educate as a response to the behavior and the severity of the consequence should match the severity of the behavior. We believe that punishment is about self-interest and collusion and therefore is inappropriate in a batterer intervention service.